Shalby Hospitals, Ahmedabad, India.
Fellowship (South Korea)
Shoulder
The shoulder is one of the largest and most complex joints in the body. The shoulder joint is formed where the humerus (upper arm bone) fits into the scapula (shoulder blade), like a ball and socket. Other important bones in the shoulder include:
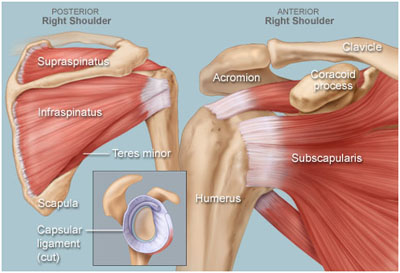
- The acromion is a bony projection off the scapula.
- The clavicle (collarbone) meets the acromion in the acromioclavicular joint.
- The coracoid process is a hook-like bony projection from the scapula.
The shoulder has several other important structures:
- The rotator cuff is a collection of muscles and tendons that surround the shoulder, giving it support and allowing a wide range of motion.
- The bursa is a small sac of fluid that cushions and protects the tendons of the rotator cuff.
- A cuff of cartilage called the labrum forms a cup for the ball-like head of the humerus to fit into.
The humerus fits relatively loosely into the shoulder joint. This gives the shoulder a wide range of motion, but also makes it vulnerable to injury.
Common Shoulder Problems
- Frozen shoulder: Inflammation develops in the shoulder that causes pain and stiffness. As a frozen shoulder progresses, movement in the shoulder can be severely limited.
- Rotator cuff tear: A tear in one of the muscles or tendons surrounding the top of the humerus. A rotator cuff tear may be a sudden injury, or result from steady overuse.
- Shoulder impingement: The acromion (edge of the scapula) presses on the rotator cuff as the arm is lifted. If inflammation or an injury in the rotator cuff is present, this impingement causes pain.
- Shoulder dislocation: The humerus or one of the other bones in the shoulder slips out of position. Raising the arm causes pain and a "popping" sensation if the shoulder is dislocated.
- Shoulder tendonitis: Inflammation of one of the tendons in the shoulder's rotator cuff.
- Shoulder bursitis: Inflammation of the bursa, the small sac of fluid that rests over the rotator cuff tendons. Pain with overhead activities or pressure on the upper, outer arm are symptoms.
- Labral tear: An accident or overuse can cause a tear in the labrum, the cuff of cartilage that overlies the head of the humerus. Most labral tears heal without requiring surgery
- Osteoarthritis: The common "wear-and-tear" arthritis that occurs with aging. The shoulder is less often affected by osteoarthritis than the knee.
Shoulder dislocation results when the top of the arm bone, the humerus, detaches from the shoulder blade, or the scapula.
Like others who suffer from frequent shoulder dislocations, you may develop the habit of self-repositioning. We highly recommend you pay us a visit to ensure proper placement. Dr. Dhaval Sagala can generally reposition the arm without anesthesia if the problem is treated quickly after the incident.
Once the area has been repositioned, he may send you home with a mobilizer sling and prescribe anti-inflammatory medication.
To prevent further dislocations arthroscopic surgery is sometimes required to stabilize the capsule of the shoulder.
Rotator Cuff Problems
The rotator cuff is a group of muscles and tendons that attach to the bones of the shoulder joint, allowing the shoulder to move and keeping it stable.
- Rotator cuff tendinitis refers to irritation of these tendons and inflammation of the bursa (a normally smooth layer) lining these tendons.
- A rotator cuff tear occurs when one of the tendons is torn from overuse or injury.
Causes
The shoulder joint is a ball and socket type joint where the top part of the arm bone (humerus) forms a joint with the shoulder blade (scapula). The rotator cuff holds the head of the humerus into the scapula and controls movement of the shoulder joint.
The tendons of the rotator cuff pass underneath a bony area on their way to attaching the top part of the arm bone. When these tendons become inflamed, they can become more frayed over this area during shoulder movements. Sometimes, a bone spur may narrow the space even more.
This problem is called rotator cuff tendinitis, or impingement syndrome, and may be due to:
- Keeping the arm in the same position for long periods of time, such as doing computer work or hairstyling
- Sleeping on the same arm each night
- Playing sports requiring the arm to be moved over the head repeatedly as in tennis, baseball (particularly pitching), swimming, and lifting weights over the head
- Working with the arm overhead for many hours or days (such as in painting and carpentry)
- Poor control or coordination of your shoulder and shoulder blade muscles
Poor posture over many years and the usual fraying of the tendons that occurs with age may also lead to rotator cuff tendinitis.
Rotator cuff tears may occur in two ways:
- A sudden or acute tear may happen when you fall on your arm while it is stretched out, or after a sudden, jerking motion when you try to lift something heavy.
- A chronic tear of the rotator cuff tendon occurs slowly over time. It is more likely in those with chronic tendinitis or impingement syndrome. At some point, the tendon wears down and tears.
There are two types of rotator cuff tears:
- A partial tear is when a tear does not completely sever the attachments to the bone.
- A complete or full thickness tear refers to a through and through tear. It may be as small as a pinpoint or all of the muscle tendon. Complete tears have detachment of the tendon from the attachment site and would not heal very well.
Symptoms
Tendinitis or Impingement Syndrome
Early on, pain occurs with overhead activities and lifting your arm to the side. Activities include brushing hair, reaching for objects on shelves, or playing an overhead sport.
- Pain is more likely in the front of the shoulder and may radiate to the side of the arm. However, this pain always stops before the elbow. If the pain travels beyond the arm to the elbow and hand, this may indicate a pinched nerve.
- There may also be pain with lowering the shoulder from a raised position.
At first, this pain may be mild and occur only with certain movements of the arm. Over time, pain may be present at rest or at night, especially when lying on the affected shoulder.
You may have weakness and loss of motion when raising the arm above your head. Your shoulder can feel stiff with lifting or movement. It may become more difficult to place the arm behind your back.
Rotator Cuff Tears
The pain with a sudden tear after a fall or injury is usually intense. Weakness of the shoulder and arm is often present, along with a snapping sensation of movement.
Symptoms of a chronic rotator cuff tear include a gradual worsening of pain, weakness, and stiffness or loss of motion. The exact point when a rotator cuff tear begins in someone with chronic shoulder tendinitis may or may not be noticed.
Most people with rotator cuff tendon tears have pain at night. Pain that is worse at night may wake you up. During the day, the pain is more tolerable and hurts with certain movements.
Over time, the symptoms become much worse and are not relieved by medicines, rest, or exercise.
Exams and Tests
A physical examination may reveal tenderness over the shoulder. Pain may occur when the shoulder is raised overhead. There is usually weakness of the shoulder when it is placed in certain positions.
X-rays of the shoulder may show a bone spur. They can be done in Dr. Dhaval Sagala's office.
If Dr. Dhaval Sagala feels you may have a rotator cuff tear, you may have one or more of the following tests:
- An ultrasound test uses sound waves to create an image of the shoulder joint. It can often show a tear in the rotator cuff.
- MRI of the shoulder may show swelling or a tear in the rotator cuff.
Sometimes, a special imaging test called arthrography is needed to diagnose a rotator cuff tear. Doctor will inject contrast material into your shoulder joint. Then an x-ray, CT scan, or MRI scan are used to take a picture of it. Contrast is usually used when Dr. Dhaval Sagala suspects a small rotator cuff tear.
Treatment
Tendinitis or Impingement Syndrome
Treatment involves resting the shoulder and avoiding activities that cause pain. It may involve:
- Ice packs applied 20 minutes at a time, 3 - 4 times a day to the shoulder
- Taking drugs like ibuprofen and naproxen to help reduce swelling and pain
- Avoiding or reducing activities that cause or worsen your symptoms to worsen
You should start physical therapy to learn exercises to stretch and strengthen the muscles of your rotator cuff.
If the pain persists or if therapy is not possible because of severe pain, a steroid injection may reduce pain and swelling in the injured tendons, to allow effective therapy.
With rest and exercise, symptoms often improve or go away. However, this may take weeks or months to occur.
Arthroscopic surgery can remove inflamed tissue and part of the bone that lies over the rotator cuff. Removing the bone may relieve the pressure on the tendons.
Rotator Cuff Tears
Rest and exercise may help someone with a partial rotator cuff tear who does not normally place a lot of demand on the shoulder. You may need surgery to repair the tendon if the rotator cuff has had a complete tear, or if the symptoms persist despite conservative therapy. Most of the time, arthroscopic surgery can be used. Some large tears require open surgery to repair the torn tendon.
Outlook (Prognosis)
Many people recover full function after a combination of medications, physical therapy, and steroid injections after an episode of rotator cuff tendinitis. Some may need to change or reduce the amount of time they play certain sports to remain pain-free.
People with tears of their rotator cuff tend to do well, although their outcome is strongly dependent upon the size of the tear and how long the tear has been present, as well as their age and pre-injury level of function.
Why is the Shoulder Unstable?
Our shoulders are the most movable joint in our bodies. However, this joint is not stable simply because of its large range of motion. It is easily injured because the ball of the upper arm is larger than the shoulder socket that holds it.
To remain stable, the shoulder is anchored by its muscles, tendons, and ligaments. Disruption of soft tissues as a result of injury, overuse or underuse of the shoulder cause problems. Another problems is the degenerative process in which tissues break down and no longer function well.
Shoulder pain may be localized or may be referred to areas around the shoulder or down the arm. Pain felt in the shoulder blade or scapula regions nearly always originate in the neck.
About shoulder dislocation
Shoulder dislocation means the head of the humerus (the ball) is completely displaced out of the glenoid (the socket). Shoulder subluxation means a 'partial dislocation' where the ball only slips out partially out of the joint and slips back into position again.
Why does the shoulder dislocate?
Shoulder is one of the most mobile and the least stable of all the joints in the body. This makes it the joint which is most vulnerable for dislocations or subluxations. In a proportion of these patients, the shoulder tends to dislocate or subluxate repeatedly after the first dislocation. Patients with a tendency for recurrent (repeated) dislocation or subluxation are said to have an unstable shoulder or shoulder instability.
How does the shoulder dislocate?
A shoulder may dislocate after a significant injury like a fall on an outstretched hand or due to a direct blow to the shoulder (traumatic dislocation), or it may dislocate without a significant injury (atraumatic dislocation) in patients who have an inherent laxity of joints (loose jointed patients). In some patients like throwing athletes, the repetitive action of forceful throwing causes the anterior capsule to stretch out and can eventually lead to a dislocation or subluxation (microtraumatic dislocation).
What are the types of shoulder dislocations?
Shoulder dislocation is classified on the basis of the direction in which the ball dislocates in relation to the socket. It is termed unidirectional if it dislocates in one direction only, or multidirectional if it dislocates in more than one direction. Thus there are the following types of dislocation:
- Unidirectional – These are usually traumatic in nature
- Anterior – the ball dislocates in front of the socket. This is the commonest type.
- Posterior – the ball dislocates behind the socket
- Inferior – the ball dislocates below the socket
- Multidirectional – These are usually atruamatic in nature and occur in patients who have inborn laxity in their joints.
What is meant by recurrent dislocation and shoulder instability?
Recurrent dislocation implies having repeated dislocations of the shoulder. Patients with a tendency for recurrent (repeated) dislocation or subluxation are said to have an unstable shoulder or shoulder instability (unstable shoulder). Shoulder instability may follow after a traumatic dislocation (after a fall or injury to the shoulder), due a generalized laxity of ligaments, or due to gradual stretching of the joint capsule due to a repetitive injury as in a throwing athlete.
Why is the shoulder joint more prone to re-dislocation (recurrent dislocation)?
The shoulder is a potentially unstable joint due the head of the humerus (ball) having a wider circumference than the socket (glenoid) which is also shallow. The stability of the shoulder is therefore dependent on the adjoining soft tissues like the labrum, capsule and the ligaments.
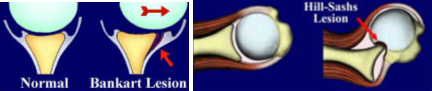
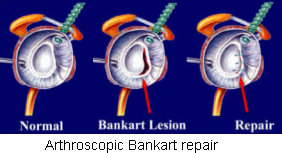
When the shoulder dislocates in the front (anterior dislocation) because of an injury, the ball (head) is forced out of the joint (socket). This causes disruption of the labrum, capsule and the ligaments in the front of the shoulder. This is known as the Bankart's lesion. The head of the humerus (ball) comes to lie over the front edge of the glenoid (socket) and this causes an indentation on the ball. This is known as the Hill-Sach's lesion.:
- Disruption of the labrum, capsule and the ligaments in the front of the shoulder. This is known as the Bankart's lesion.
- The head of the humerus (ball) comes to lie over the front edge of the glenoid (socket) and this causes an indentation on the ball. This is known as the Hill-Sach's lesion.
In a proportion of patients the Bankart Bankart's lesion does not heal completely causing the joint to be unstable and vulnerable to further dislocation with lesser injury (trivial trauma) trivial or no injury. It is now well known has been shown that the younger the patient at the time of first dislocation (age less than 25 years), higher is the chance of a re-dislocation. The chance of shoulder re-dislocating after the first dislocation can be as high as 70-90% in a young patient (below 25 yrs of age). With each dislocation the capsule in the front gets stretched and thinned out making further dislocations to happen occur with relative ease.
On the other hand, in In patients with an inherent laxity of the joint capsule, the joint is capacious (lax) and is easily dislocated with trivial injury or during activities like throwing or wearing a shirt.
How do you diagnose shoulder instability?
Shoulder instability is diagnosed on the basis of patient's symptoms and physical examination. Shoulder instability could present with history of repeated episodes frank dislocations or as episodes of subluxations (partial dislocations) causing pain or discomfort.
A patient with recurrent dislocating tendency may have suffered a dislocation after an injury, following which repeated dislocations occur with relative ease (without any significant injury).present with a history of more than one episode of dislocation (usually a few) occurring following an episode of "first dislocation" occurring after a significant injury with subsequent dislocations occurring "with ease". Most of these patients are able to reduce (put back the dislocated shoulder) on their own or with some assistance.
Patients with repeated episodes of subluxations will present Some patients may present with pain or discomfort while moving the shoulder without an obvious dislocation. This is due to the shoulder being subluxed (partially dislocated) instead of a complete dislocation. This usually occurs in the throwing position (abduction and external rotation of the arm) in athletes or while doing activities of daily living like putting on a shirt or lifting a heavy object. Physical examination will reveal an otherwise normal shoulder. The only positive finding is the 'apprehension test'. In this test the arm is put in the vulnerable position of abduction and external position. This will cause pain or discomfort and the patient becomes apprehensive that the shoulder will re-dislocate.
In patients with ligament laxity, episodes of dislocation or subluxation will occur without any significant injury. Further, since they have generalized ligament laxity, they may present with symptoms in both shoulders (bilateral dislocations or subluxations). Also these patients may exhibit evidence of laxity (loose-jointed) in the form of repeated patellar (knee cap) dislocations or hyper-extended knees. These patients will also have a positive 'apprehension test' on examination.
Are there any tests which help in diagnosis a patient with shoulder instability?
There are certain tests which may be performed to gain further information and plan out the treatment.
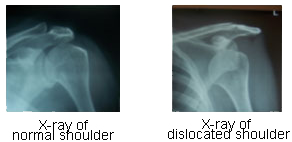
- Plain X-rays: These are helpful only in patients with a frank dislocation where it demonstrates the presence of a dislocated head. In cases with recurrent dislocation certain special views will demonstrate the Hill-Sach's lesion (indentation at the back of the head). Otherwise X-rays are not of much value.
- MRI / MR Arthrography: This will clearly demonstrate the Bankart lesion (which is diagnostic of a recurrent dislocation) as well as the Hill-Sach lesion. In patients with ligament laxity, arthrography reveals a very capacious joint with a lax capsule.
- CT / CT arthrography: This is very useful in demonstrating any bone loss in the glenoid socket. The amount of bone loss in the glenoid will dictate the type of surgical procedure to be performed.
Treatment of shoulder dislocation and instability (Bold print)
What is treatment of a 'First-time dislocation' of the shoulder?
When a shoulder dislocates it must be promptly relocated by closed reduction (manipulating the shoulder without the need for open surgery). This may require a general anaesthetic or some form of sedation. Once the shoulder is relocated, the arm is immobilized by the side of the chest using a shoulder immobilizer type of sling for a period of 3-6 weeks. In very young patients (below the age of 25 years) and high demand athletes, there may be a case need for surgery (Bankart repair) immediately after the first dislocation to prevent the chance of further dislocations as the incidence of recurrent dislocation in these patients is very high.
What is treatment of recurrent dislocation or instability of the shoulder?
The treatment options for repeated shoulder dislocations depend on the functional demands of the patient and the level of disability suffered by the patient due to these episodes of instability.
- Conservative (Non-surgical) treatmentEvery patient with shoulder instability may not require surgery. Those patients who have a sedentary life-style and those who are not involved in strenuous activities or active sports may be able to manage without surgery as long as they are able to restrict activities which are likely to cause a dislocation or subluxation. However, there is an ever present risk of dislocation or symptomatic instability occurring at any point in time if the shoulder is placed in a vulnerable position.
- Surgery
Most young patients and those involved with any type of active sport are likely to need surgery to stabilize their unstable shoulder. The commonly used surgical options are:
Arthroscopic Bankart repair (Key-hole surgery)
This is performed through 3 small holes (called portals). The Bankart repair involves re-attaching the detached capsulo-labral complex to the glenoid using suture anchors. It is also possible to do a capsular shift (tightening of the lax capsule) at the same time. The advantage of the arthroscopic technique is its minimally invasive nature which minimizes morbidity of surgery and hospital stay. Further it allows excellent visualization of the entire shoulder joint and is very useful in detecting and treating other causes of dislocation like an ALPSA lesion as well as associated pathology like a SLAP lesion.
Open Bankart repair
The Bankart repair and capsular shift is can also be performed by open surgery which involves making a cut of about 3-5 cm. over the front of the shoulder. This procedure also involves cutting through the subscapularis muscle which needs to be repaired at the end of the procedure.
Bony operations
In cases where there is significant bone loss in the glenoid or a large Hill-Sach's lesion (engaging Hill-Sach's), a Bankart repair alone is likely to fail. In such situations a Bristow-Latarjet procedure (transfer of coracoid process to the glenoid defect) or a bone graft to the Hill-Sach's lesion needs to be performed. These procedures require an open operation.
Post-operative course after surgery
The patient may leave the hospital on the same day or the next day in case of an arthroscopic repair, and after 2-3 days after open surgery. The arm is placed in a shoulder immobilizer type of sling which restricts movement of the arm upwards, outwards and outward rotation of the arm. Depending upon the type of surgery performed and the strength of the repair achieved, the arm will be immobilized in the sling for a period of 3- 6 weeks. At around 2-3 weeks after surgery, pendulum exercises (gravity assisted movements of the arm) are initiated. At around 6 weeks after surgery, full range-of-motion exercises as well as shoulder strengthening exercises are started.
When can one return to routine activities and sporting activities?
Overall it will take around 2-3 months after surgery for any patient to return to pre-operation status as far routine day-to-day activities are concerned. It may take around 3-4 months for a recreational athlete to return to sports, and even longer for a professional athlete (depending upon the nature of sport and the level of competition involved).